The development of antibody-drug conjugates (ADCs) has transformed cancer treatment by combining the specificity of monoclonal antibodies with the cytotoxic potency of chemotherapy agents. Gemtuzumab ozogamicin (GO) was the first ADC to receive FDA approval, marking a significant milestone in targeted oncology therapies. Initially approved in 2000 for relapsed/refractory acute myeloid leukemia (AML), GO was withdrawn in 2010 due to safety concerns. However, subsequent clinical trials using a fractionated dosing regimen demonstrated improved efficacy and reduced toxicity, leading to its re-approval in 2017. It is now sold under the brand name Mylotarg®. This article reviews the history, mechanism of action, clinical development, and impact of GO on AML treatment.
CD33 is a transmembrane receptor expressed on myeloid lineage cells and myeloblasts in over 80% of AML cases, making it a suitable target for therapy. Unlike normal hematopoietic stem cells, which lack CD33 expression, leukemic blasts express high levels of the antigen, allowing selective targeting while sparing normal progenitor cells.
GO consists of a recombinant humanized IgG4 kappa monoclonal antibody directed against CD33, conjugated to a cytotoxic derivative of calicheamicin via a cleavable linker. The antibody component enables selective binding to CD33+ AML cells, while the cytotoxic payload induces DNA damage and apoptosis.
Binding and Internalization: GO binds to CD33 on AML cells and is internalized via endocytosis.
Intracellular Processing: The conjugate is transported to lysosomes, where the acidic environment cleaves the linker.
Cytotoxic Effect: The released calicheamicin binds to DNA, causing double-strand breaks, leading to cell cycle arrest and apoptosis.
This mechanism provides targeted cytotoxicity, reducing off-target effects associated with conventional chemotherapy.

GO’s clinical efficacy was first demonstrated in three Phase 2 studies evaluating its use as a monotherapy in adult patients with first-relapse AML. These studies showed an overall response rate (ORR) of 26%, with complete remission (CR) or CR with incomplete hematologic recovery (CRi) achieved in 13% of patients. The median relapse-free survival (RFS) was 5.2 months, with responders experiencing a median overall survival (OS) of 12.6 months.
Based on these results, GO received accelerated FDA approval in 2000 for adult RR-AML patients. The approval was contingent on confirmatory post-marketing studies to validate long-term efficacy and safety.
Subsequent studies expanded GO’s approval to pediatric AML. Phase 1/2 trials demonstrated an ORR of 28%, leading to its use in pediatric RR-AML patients aged two years and older.
To evaluate GO’s efficacy in newly diagnosed AML, the SWOG-S0106 Phase 3 trial compared standard induction chemotherapy (cytarabine/daunorubicin) with or without GO. The study was halted early due to increased early mortality in the GO arm (5.5% vs. 1.4% in controls), driven primarily by hemorrhagic and infectious complications.
The lack of significant improvement in response rates or survival outcomes, combined with concerns about hepatotoxicity and veno-occlusive disease (VOD), led to the voluntary withdrawal of GO from the market in 2010.
Following its withdrawal, researchers investigated whether adjusting GO’s dosing schedule could preserve efficacy while reducing toxicity. The fractionated dosing regimen—administering 3 mg/m² on Days 1, 4, and 7—allowed better saturation of CD33 receptors while avoiding excessive peak plasma concentrations that contributed to hepatotoxicity.
Evaluated GO monotherapy using fractionated dosing in first-relapse AML.
ORR of 33%, with a median relapse-free survival of 11 months.
No VOD cases, supporting improved safety profile.
GO + chemotherapy improved event-free survival (EFS) compared to chemotherapy alone.
Median EFS: 15.6 months (GO) vs. 9.7 months (control).
Significant reduction in relapse risk in patients with favorable/intermediate cytogenetics.
Compared GO monotherapy vs. best supportive care.
GO significantly improved overall survival (OS): 4.9 months (GO) vs. 3.6 months (control).
These studies demonstrated that fractionated GO dosing reduced toxicity while maintaining efficacy, leading to FDA re-approval in 2017.

The incidence of VOD, a major concern with the original GO dosing, was significantly reduced with the fractionated regimen. In the ALFA-0701 trial, VOD occurred in only 5% of patients, compared to rates as high as 40% in earlier studies.
GO-induced myelosuppression led to prolonged cytopenias and increased hemorrhagic risk, necessitating close monitoring and supportive care.
Premedication with corticosteroids and antihistamines is required to prevent infusion-related hypersensitivity reactions.
GO is now incorporated into standard AML treatment in the following settings:
ND-AML (Favorable/Intermediate Cytogenetics): In combination with chemotherapy.
RR-AML (Pediatric and Adult Patients): As monotherapy.
Unfit ND-AML (Elderly Patients): As a single-agent therapy.
The approval of GO, along with targeted agents like midostaurin (FLT3 inhibitor), enasidenib (IDH2 inhibitor), and CPX-351 (liposomal cytarabine/daunorubicin), highlights the importance of rapid genetic profiling in AML to personalize treatment.
GO + venetoclax/HMA for older AML patients.
GO + multi-agent salvage chemotherapy for RR-AML.
Ongoing trials exploring GO with novel targeted therapies.

Improved linker chemistries enhancing payload stability and release.
Alternative cytotoxic payloads for increased selectivity.
Expansion beyond CD33 to other AML targets (e.g., CD123, CLL-1).
Combinations with checkpoint inhibitors or bispecific antibodies.
Potential synergy between ADCs and immune-modulating agents.

Gemtuzumab ozogamicin remains a pivotal ADC in oncology, illustrating the importance of refining dosing strategies to optimize safety and efficacy. Its re-approval underscores the evolving landscape of AML therapy, where biomarker-driven approaches and targeted agents are reshaping treatment paradigms. As next-generation ADCs continue to emerge, lessons from GO’s development will inform future strategies for precision oncology.
Related: ADC Payloads: Expanding Beyond Microtubules and DNA-Damaging Agents
At Biointron, we are dedicated to accelerating antibody discovery, optimization, and production. Our team of experts can provide customized solutions that meet your specific research needs, including antibody-drug conjugates from Abinvivo. Contact us to learn more about our services and how we can help accelerate your research and drug development projects.
References:
Baron, J., & Wang, E. S. (2018). Gemtuzumab Ozogamicin for Treatment of Acute Myeloid Leukemia. Expert Review of Clinical Pharmacology, 11(6), 549. https://doi.org/10.1080/17512433.2018.1478725
For an antibody candidate, strong target binding is only part of the path toward……
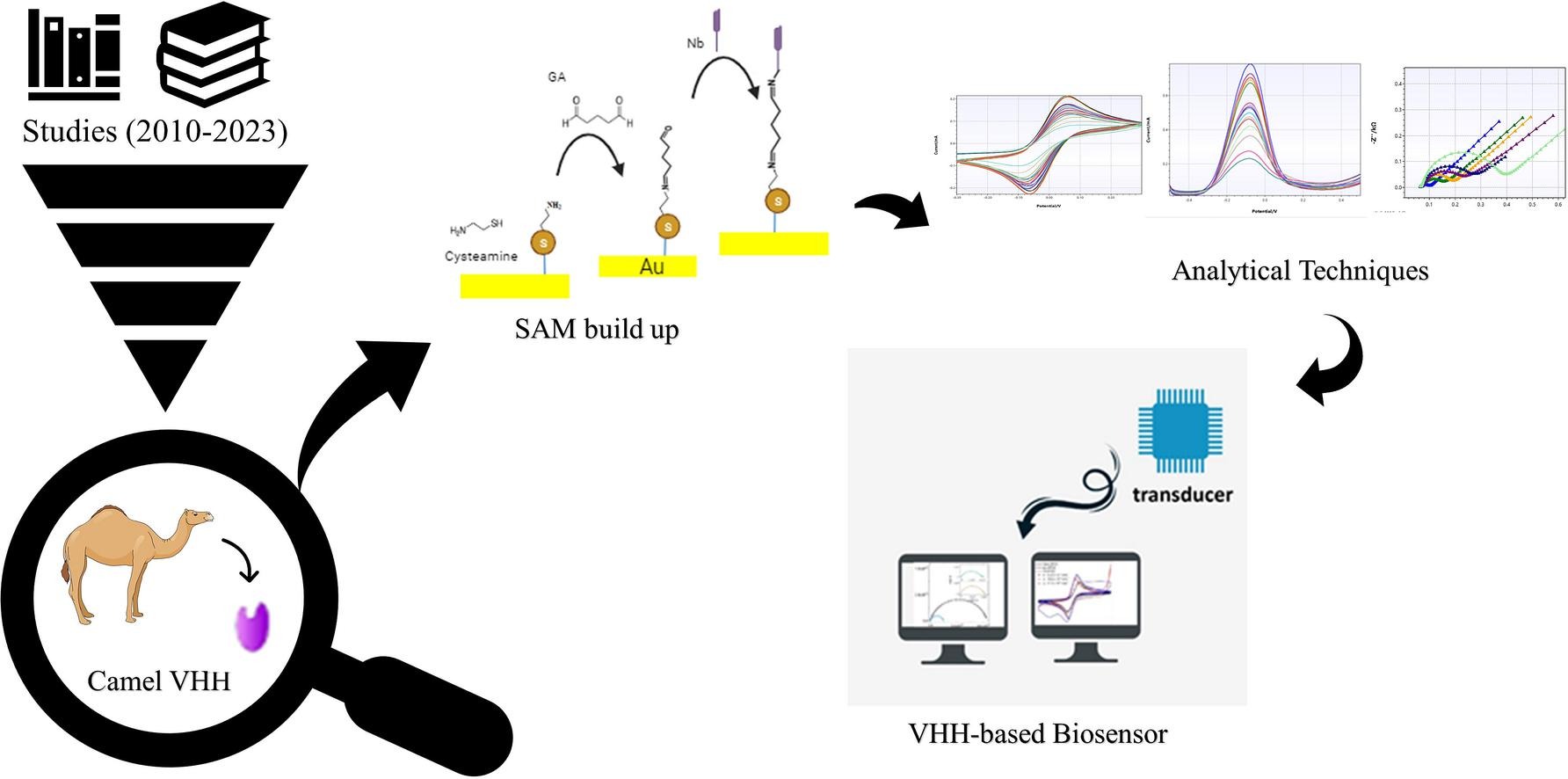
Explore VHH-based biosensors for high-sensitivity detection using nanobodies in ……
Biointron’s Antibodies After Hours: BIO 2026 Reception was held at The Lion's Sh……
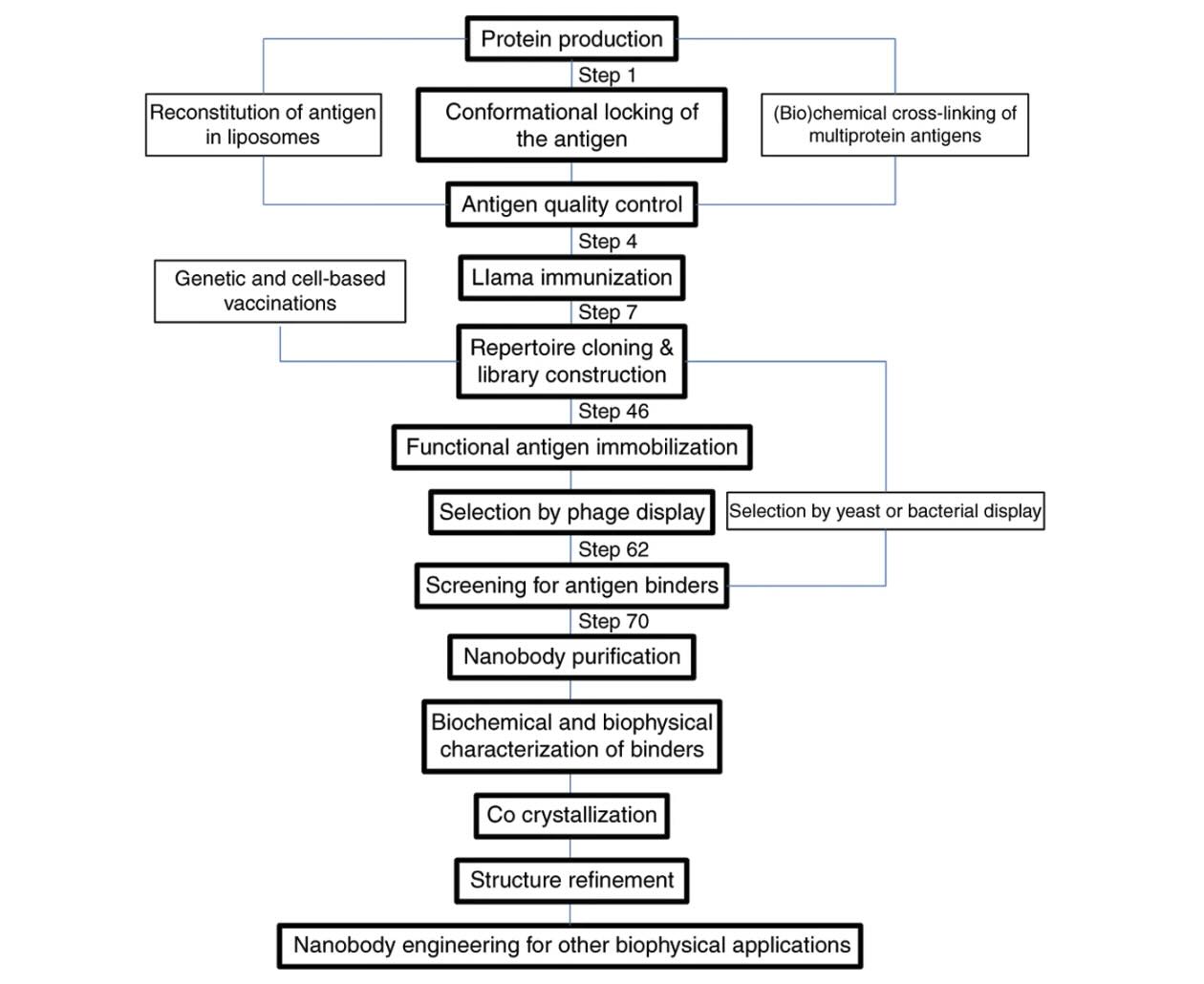
Explore how VHH antibodies stabilize protein conformations for crystallography, ……