The past 25 years have seen significant advancements in therapeutic antibodies for cancer treatment, driven by academic and industrial collaborations. From the approval of rituximab in 1997 to the development of immune checkpoint inhibitors and bispecific antibodies, oncology has witnessed a transformation in drug discovery and regulatory approvals. The European Medicines Agency (EMA) and the U.S. Food and Drug Administration (FDA) have played large roles in shaping this landscape, particularly over the past decade, as antibody-drug conjugates (ADCs) and bispecific antibodies (BsAbs) have gained traction. A recent review highlights six pivotal events that have defined the development and approval of antibody-based oncology therapies.1

In the 1990s, cancer treatment was largely dependent on chemotherapy, which often caused significant toxicity with limited efficacy. The hybridoma technology developed in the 1970s allowed the creation of monoclonal antibodies, but their clinical utility was initially uncertain due to immunogenicity concerns.
A breakthrough came when researchers at Stanford University identified CD20 as a viable target for B-cell malignancies. Collaborating with IDEC Pharmaceuticals, they developed a chimeric monoclonal antibody, IDEC-C2B8, later named rituximab. The antibody combined a murine variable region with a human constant region, reducing immunogenicity while retaining efficacy.
Rituximab is a chimeric monoclonal antibody composed of human IgG1 constant regions and murine variable regions that specifically bind to the CD20 antigen. CD20 is a transmembrane protein expressed on B cells from the pre-B cell stage to maturity but is absent on stem cells and plasma cells. Binding of rituximab to CD20 induces B-cell depletion through multiple mechanisms, including:
Antibody-dependent cellular cytotoxicity (ADCC)
Complement-dependent cytotoxicity (CDC)
Direct apoptosis
Antibody-dependent phagocytosis (ADP)
Clinical trials in B-cell lymphomas showed significant tumor regression, leading to FDA approval in 1997. Rituximab not only provided a new therapeutic strategy for hematologic cancers but also established the paradigm of targeted immunotherapy. Its approval paved the way for subsequent anti-CD20 therapies, including ofatumumab and obinutuzumab, and expanded the use of monoclonal antibodies in oncology.
Related: Rituximab: The First Monoclonal Antibody Approved for Cancer Treatment

While rituximab revolutionized lymphoma treatment, solid tumors posed a greater challenge due to their immunosuppressive microenvironment. In 1987, researchers at UCLA discovered that approximately 25% of breast cancers overexpressed the HER2 oncogene, correlating with poor prognosis.
Scientists generated a humanized anti-HER2 monoclonal antibody, trastuzumab, to target HER2-positive breast cancer. Initial hesitation from Genentech's management delayed clinical trials, but advocacy from oncologists and patient groups pushed the program forward.
HER2, a transmembrane tyrosine kinase receptor, is overexpressed in approximately 15-20% of breast cancers. Overexpression of HER2 is associated with increased tumor aggressiveness, higher rates of metastasis, and shorter survival. Trastuzumab, a monoclonal antibody, binds specifically to the extracellular domain of the HER2 receptor, inhibiting its downstream signaling pathways. This mechanism leads to several therapeutic effects:
Suppression of tumor proliferation by blocking HER2-mediated growth signals.
Antibody-dependent cellular cytotoxicity (ADCC)
Clinical trials demonstrated significant survival benefits, leading to FDA approval in 1998. The success of trastuzumab led to the development of other HER2-targeting therapies, including pertuzumab, ADCs like trastuzumab emtansine, and bispecific antibodies. The approval of trastuzumab reinforced the principle that targeted antibody therapy could be effective against solid tumors.
Related: Trastuzumab: Transforming the Landscape of Breast Cancer Treatment

While monoclonal antibodies like rituximab and trastuzumab provided targeted therapy, their efficacy depended on mechanisms such as antibody-dependent cellular cytotoxicity (ADCC) and complement activation. Researchers sought to enhance antibody potency by conjugating cytotoxic drugs to antibodies, leading to the development of ADCs.
Gemtuzumab ozogamicin was the first ADC approved for acute myeloid leukemia (AML). The antibody component targeted CD33, a marker on AML cells, while the cytotoxic payload, calicheamicin, induced DNA damage upon internalization. The ADC demonstrated efficacy in AML patients, leading to accelerated FDA approval in 2000.
However, post-approval studies raised concerns about toxicity, resulting in voluntary withdrawal in 2010. Subsequent trials demonstrated that lower, fractionated dosing improved safety and efficacy, leading to its re-approval in 2017. Gemtuzumab ozogamicin established the feasibility of ADCs, paving the way for other ADC approvals, including brentuximab vedotin and trastuzumab deruxtecan.
Related: Antibody-Drug Conjugates: Transforming the Biopharma Landscape

Traditional monoclonal antibodies activate immune cells through Fc receptor interactions, but this mechanism does not effectively engage T cells, which lack Fc receptors. Bispecific antibodies (BsAbs) were developed to bridge this gap by simultaneously binding tumor-associated antigens and T cells.
Blinatumomab, a bispecific T-cell engager (BiTE), was engineered to link CD19 on B-cell malignancies with CD3 on T cells, activating cytotoxic T-cell responses. The antibody was produced using CHO cells, ensuring stability and scalability for clinical use.
Due to concerns about cytokine release syndrome (CRS), researchers conducted preclinical safety studies in chimpanzees before initiating human trials. Blinatumomab demonstrated strong efficacy in B-cell acute lymphoblastic leukemia (B-ALL), leading to FDA approval in 2014.
The approval of blinatumomab accelerated interest in bispecific antibodies, leading to the development of newer formats such as the DuoBody and BiTEs, which now include multiple FDA-approved agents for hematologic and solid tumors.
Related: Bispecific Antibodies in Cancer Therapy: Engineering, Mechanisms, and Clinical Applications

Checkpoint inhibitors revolutionized oncology by shifting the focus from direct tumor targeting to immune system modulation. The discovery of CTLA-4 as a negative regulator of T-cell activation in the 1980s laid the foundation for checkpoint blockade therapy.
Medarex developed ipilimumab, an anti-CTLA-4 antibody, to enhance T-cell-mediated anti-tumor responses. Despite initial skepticism, clinical trials demonstrated long-term survival benefits in melanoma patients, leading to FDA approval in 2011.
The success of ipilimumab encouraged further development of immune checkpoint inhibitors, including anti-PD-1 and anti-PD-L1 antibodies such as nivolumab and pembrolizumab, which have since been approved for multiple cancer types.
Related: Therapeutic Targets - Immune Checkpoint Inhibitors

Traditionally, cancer drugs were approved based on tumor origin (e.g., breast or lung cancer). This changed with pembrolizumab, an anti-PD-1 antibody, which received the first tissue-agnostic FDA approval in 2017.
The approval was based on studies showing that tumors with high microsatellite instability (MSI-high) responded to pembrolizumab regardless of cancer type. This marked a shift toward biomarker-driven therapy rather than organ-based classification.
Following pembrolizumab’s success, other tissue-agnostic approvals have followed, including trastuzumab deruxtecan for HER2-expressing solid tumors. The trend toward biomarker-based approvals continues to reshape oncology drug development.
Related: HTP Recombinant Antibody Production

These events have shaped antibody-based drug development, setting the stage for continued innovation in oncology. Advances in ADCs, bispecific antibodies, and immune checkpoint inhibitors have expanded treatment options for patients, with newer formats such as multi-specific antibodies and antibody-mimetics poised to further enhance therapeutic efficacy. The close collaboration between academia and industry remains crucial in driving the next generation of antibody therapies.
At Biointron, we are dedicated to accelerating antibody discovery, optimization, and production. Our team of experts can provide customized solutions that meet your specific research needs, including HTP Recombinant Antibody Production, Bispecific Antibody Production, Large Scale Antibody Production, and Afucosylated Antibody Expression. Contact us to learn more about our services and how we can help accelerate your research and drug development projects.
Paul, S., & Zhou, S. (2025). Six events that shaped antibody approvals in oncology. Frontiers in Immunology, 16, 1533796. https://doi.org/10.3389/fimmu.2025.1533796
For an antibody candidate, strong target binding is only part of the path toward……
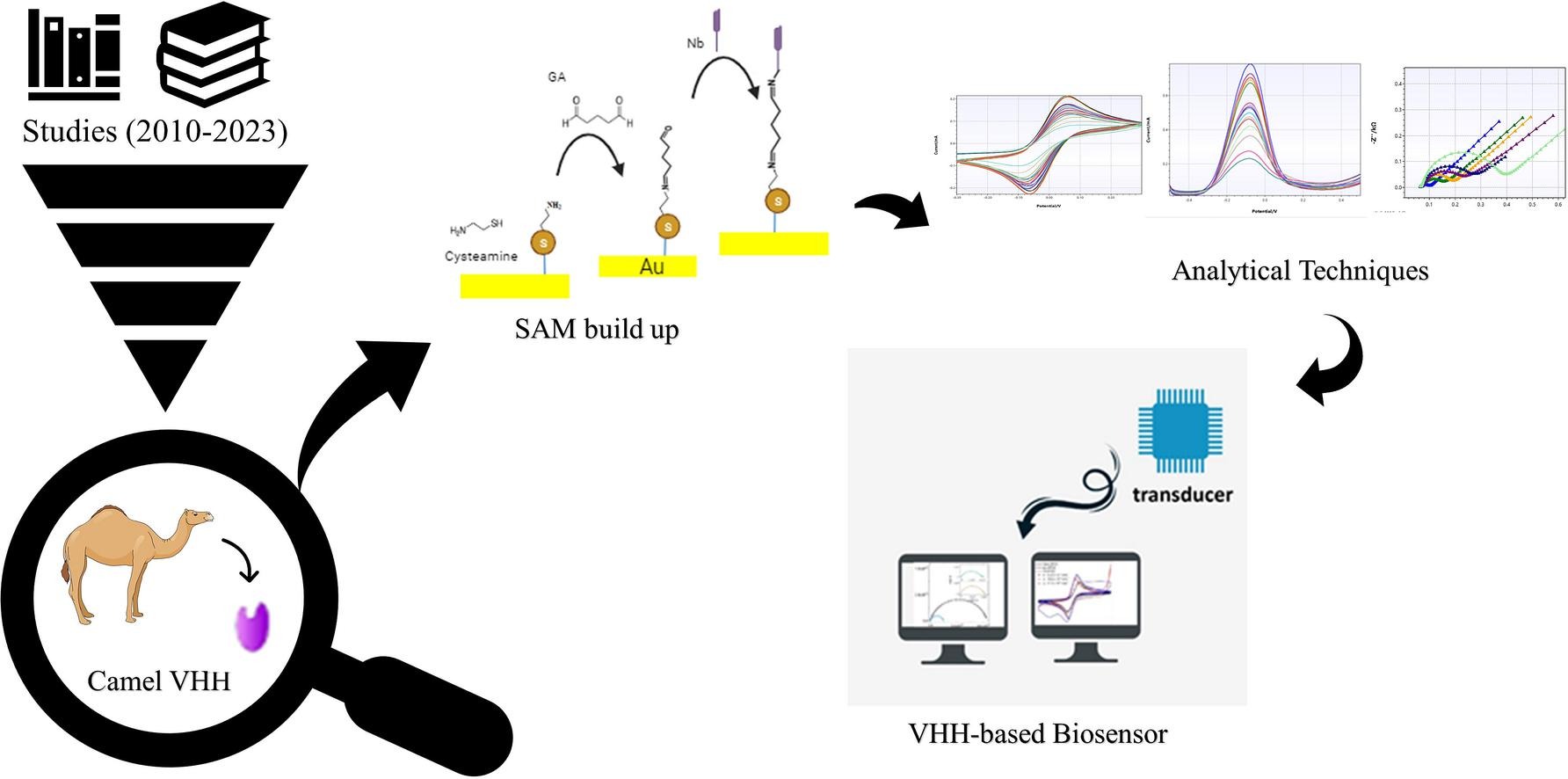
Explore VHH-based biosensors for high-sensitivity detection using nanobodies in ……
Biointron’s Antibodies After Hours: BIO 2026 Reception was held at The Lion's Sh……
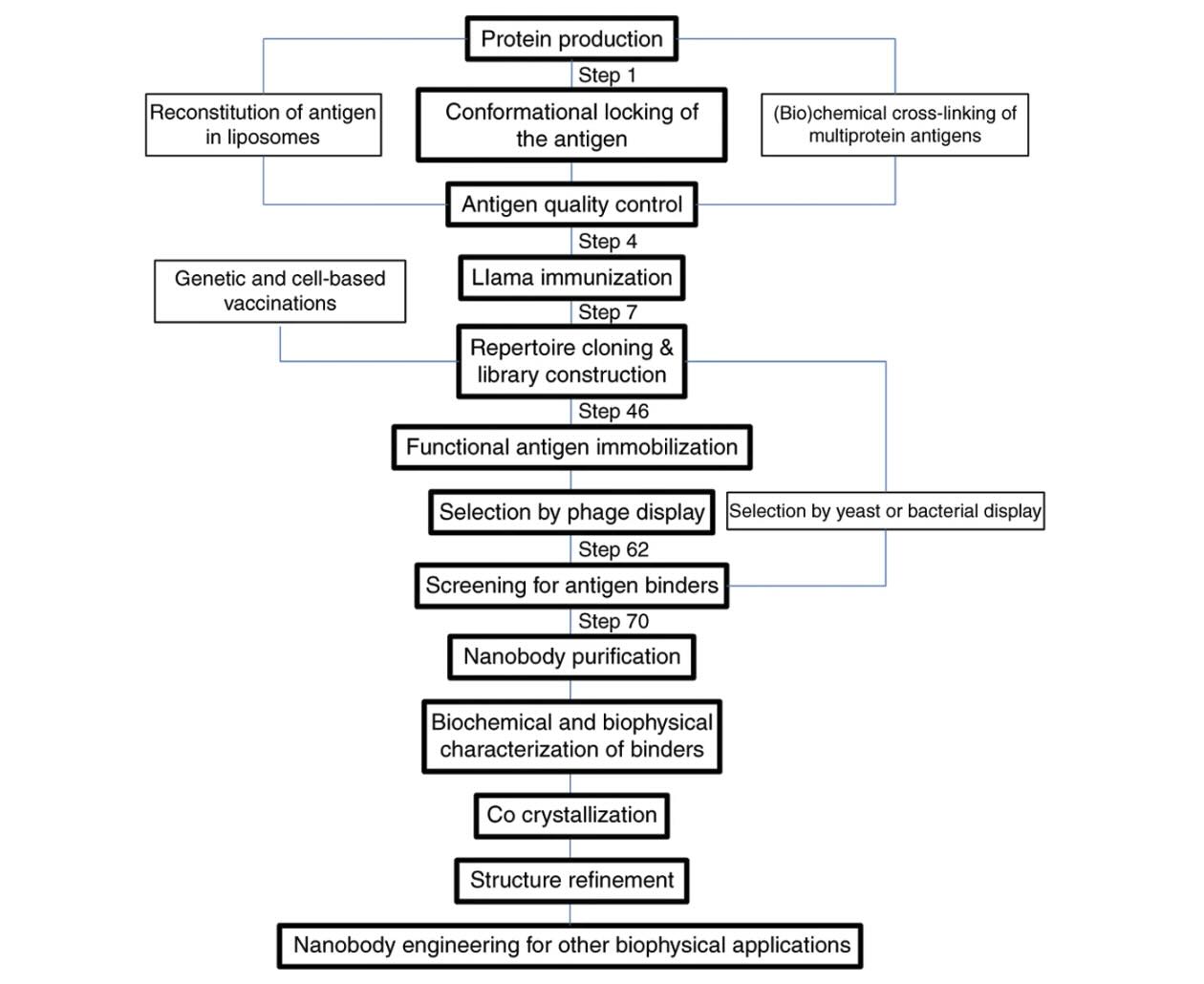
Explore how VHH antibodies stabilize protein conformations for crystallography, ……