Antibody-drug conjugates (ADCs) represent a transformative class of targeted cancer therapies that combine the specificity of monoclonal antibodies (mAbs) with the potent cytotoxicity of small-molecule drugs. Through this structure, ADCs aim to selectively deliver chemotherapy to cancer cells while minimizing damage to healthy tissues.
The FDA approval of ADCs such as Brentuximab vedotin (Adcetris®) and Trastuzumab emtansine (Kadcyla®, T-DM1) validated the ADC approach and catalyzed the expansion of this modality. Since then, newer generations like Trastuzumab deruxtecan (Enhertu®) and Sacituzumab govitecan (Trodelvy®) have redefined the boundaries of target expression and payload design. As of 2025, more than 80 ADC candidates are under clinical investigation across hematologic malignancies and solid tumors.

Despite these advances, ADCs still face challenges, including drug-to-antibody ratio (DAR) optimization, off-target toxicity, resistance mechanisms, and scalable manufacturing. This article reviews the mechanism of action, clinical development, design considerations, and future trends in ADC technology.
The activity of an ADC depends on a sequence of biological events that ensure selective tumor killing:
The mAb component of the ADC binds to a tumor-associated antigen that is overexpressed on cancer cells but limited on normal tissues. Ideal targets are internalizing and tumor-specific, such as:
HER2 (breast/gastric cancer)
CD30 (lymphomas)
TROP2, Nectin-4, and MUC16 (solid tumors)
CD22, CD123, and CD33 (hematologic cancers)
Target selection directly affects the efficacy and safety profile of an ADC.

Once the ADC binds its target, it is internalized into the cancer cell via receptor-mediated endocytosis. The internalization efficiency influences payload delivery and therapeutic effect. ADCs targeting rapidly internalizing receptors generally show superior cytotoxicity.
Following endocytosis, the ADC is trafficked to the lysosome. Here, the linker is cleaved enzymatically (for cleavable linkers) or the entire antibody is degraded (for non-cleavable linkers), releasing the active drug intracellularly.
The released payload then induces cell death. Payloads typically include:
Microtubule inhibitors (e.g., MMAE, MMAF, DM1): arrest mitosis and promote apoptosis.
DNA-damaging agents (e.g., calicheamicin, PBD dimers): cause DNA breaks and replication stress.
Topoisomerase I inhibitors (e.g., DXd, SN-38): inhibit DNA unwinding during replication.
Many payloads also produce a bystander effect, diffusing into nearby tumor cells and amplifying the antitumor activity.

Over the past decade, ADCs have steadily gained FDA approvals. Examples include:
Adcetris® (Brentuximab vedotin): Targets CD30; approved for Hodgkin lymphoma and ALCL.
Kadcyla® (Trastuzumab emtansine): HER2-positive breast cancer.
Enhertu® (Trastuzumab deruxtecan, DS-8201): Redefined HER2 targeting by demonstrating efficacy in HER2-low breast and gastric cancers.
Trodelvy® (Sacituzumab govitecan): TROP2-targeting ADC approved for triple-negative breast cancer and urothelial carcinoma.
Elahere® (Mirvetuximab soravtansine-gynx): For folate receptor alpha (FRα)-positive platinum-resistant ovarian cancer.
Zynlonta® (Loncastuximab tesirine-lpyl): For relapsed or refractory large B-cell lymphoma.
Emrelis™ (Telisotuzumab vedotin-tllv): Approved in 2025 for the treatment of c-Met overexpressing non-small cell lung cancer (NSCLC). It is indicated for patients with metastatic or locally advanced NSCLC who have received prior therapy, representing a targeted option for EGFR-mutated, c-Met+ tumors.
Datroway™ (Datopotamab deruxtecan-dlnk): A next-generation TROP2-targeting ADC with a DXd payload, approved for two major indications in 2025:
EGFR-mutated non-small cell lung cancer (NSCLC): For patients with metastatic or locally advanced NSCLC harboring EGFR mutations, who have previously received EGFR-directed therapy and platinum-based chemotherapy.
HR-positive, HER2-negative breast cancer: For patients with unresectable or metastatic disease who have progressed after endocrine-based therapy and chemotherapy.
Built on the same platform as Enhertu, Datroway represents the growing clinical success of DXd-based, high-DAR ADCs with improved tolerability.
These approvals reflect the diversification of ADC applications across histologies and molecular profiles, with better payload chemistry and broader patient benefit.
Over 80 ADCs are in clinical development. Notable trends include:
Exploration of new targets such as DLL3, Mesothelin, GPR20, and PTK7.
Applications in glioblastoma, pancreatic cancer, NSCLC, and prostate cancer.
Combinations with immune checkpoint inhibitors and targeted kinase inhibitors.
The development focus has also shifted toward tumor microenvironment-responsive linkers and non-oncology indications.
The antibody should:
Bind the tumor antigen with high affinity.
Induce internalization efficiently.
Have low immunogenicity (humanized or fully human).
Maintain long half-life and low off-target binding.
Engineering the Fc domain (e.g., to silence ADCC/CDC) may further reduce immunotoxicity.
Linkers determine when and where the payload is released. Two major types:
Cleavable linkers (e.g., valine-citrulline): Stable in circulation; cleaved by lysosomal enzymes or acidic pH.
Non-cleavable linkers (e.g., thioether): Require full antibody degradation; release payload as a conjugated complex.
Proper linker design balances stability, efficacy, and the bystander effect.
Common payload classes include:
Auristatins (MMAE, MMAF): Microtubule depolymerization.
Maytansinoids (DM1, DM4): Mitosis disruption.
PBD dimers, calicheamicin: DNA crosslinking.
Topoisomerase I inhibitors (e.g., DXd in Enhertu, SN-38 in Trodelvy): Emerging as favorable for solid tumors.
Ideal payloads should be membrane-permeable, potent (sub-nanomolar IC50), and stable until release.
DAR represents the average number of payloads per antibody. Traditional wisdom holds that:
Low DAR (<2) = insufficient potency.
High DAR (>4–6) = increased aggregation, faster clearance, off-target effects.
Optimal DAR (2–4) = balance between efficacy and pharmacokinetics.
Recent evidence suggests that high DAR designs are viable when coupled with low-toxicity payloads and optimized linkers. For example, Enhertu (DS-8201) employs a DAR of ~8 with a membrane-permeable, low-toxicity topoisomerase I inhibitor (DXd), enabling:
Potent bystander effect
Low systemic toxicity
Strong efficacy even in low HER2-expressing tumors
This shift challenges previous limitations on DAR and opens new strategies in ADC design.

Traditional conjugation (e.g., lysine or cysteine-based) leads to heterogeneous ADCs. Modern technologies improve reproducibility and efficacy:
Cysteine re-bridging
Unnatural amino acid incorporation
Enzyme-mediated ligation (e.g., Sortase A, transglutaminase)
Glycan engineering at Fc N297 site
These methods allow precise control over DAR, linker position, and stability.
Despite their promise, ADCs face persistent limitations:
Off-target toxicity: Due to low-level antigen expression in healthy tissues or premature drug release.
Resistance mechanisms: Including antigen downregulation, altered internalization, lysosomal sequestration, or drug efflux (e.g., MDR1).
Tumor heterogeneity: Not all cancer cells express the target antigen.
Manufacturing complexity: Especially for site-specific or high-DAR ADCs at commercial scale.
Comprehensive preclinical evaluation and biomarker-guided patient selection are essential.
Key innovation areas include:
Bispecific ADCs (BsADCs): Dual-antigen targeting to improve selectivity and overcome resistance.
Immune-stimulatory ADCs: Combining ADCs with STING agonists or immune checkpoint inhibitors.
ADC-radioconjugates: Incorporating radionuclides for theranostic applications.
Non-oncology ADCs: Investigational use in autoimmune diseases and infections.
Modular ADC platforms: Faster, flexible ADC generation using standardized payload-linker modules.
ADC innovation is expanding beyond traditional cytotoxins into the broader world of targeted biologics.
Antibody-drug conjugates continue to redefine cancer treatment by combining precise targeting with potent cytotoxic payloads. With ongoing advances in antibody engineering, linker chemistry, site-specific conjugation, and payload design, ADCs are poised for broader impact—not only in oncology but potentially in other disease areas. Emerging strategies like high-DAR/low-toxicity design, bispecific ADCs, and immune-modulatory combinations will shape the next generation of ADC therapeutics.
Gao Y, Xia Y, Chen Y, Zhou S, Fang Y, Yu J, Zhang L, Sun L. Key considerations based on pharmacokinetic/pharmacodynamic in the design of antibody-drug conjugates. Front Oncol. 2025 Jan 9;14:1459368. doi: 10.3389/fonc.2024.1459368. PMID: 39850824; PMCID: PMC11754052.
Baah, S.; Laws, M.; Rahman, K.M. Antibody–Drug Conjugates—A Tutorial Review. Molecules 2021, 26, 2943. https://doi.org/10.3390/molecules26102943
Zhou, Q. Site-Specific Antibody Conjugation for ADC and Beyond. Biomedicines 2017, 5, 64. https://doi.org/10.3390/biomedicines5040064
https://www.fda.gov/drugs/development-approval-process-drugs/novel-drug-approvals-fda
Fu, Z., Li, S., Han, S. et al. Antibody drug conjugate: the “biological missile” for targeted cancer therapy. Sig Transduct Target Ther 7, 93 (2022). https://doi.org/10.1038/s41392-022-00947-7
Modi S, Saura C, Yamashita T, Park YH, Kim SB, Tamura K, Andre F, Iwata H, Ito Y, Tsurutani J, et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. New England Journal of Medicine, 2022, 387(1): 9 – 20. https://doi.org/10.1056/NEJMoa2203690
Joubert N, Beck A, Dumontet C, Denevault-Sabourin C. Antibody-Drug Conjugates: The Last Decade. Pharmaceuticals (Basel). 2020 Sep 14;13(9):245. doi: 10.3390/ph13090245. PMID: 32937862; PMCID: PMC7558467.
For an antibody candidate, strong target binding is only part of the path toward……
Explore VHH-based biosensors for high-sensitivity detection using nanobodies in ……
Biointron’s Antibodies After Hours: BIO 2026 Reception was held at The Lion's Sh……
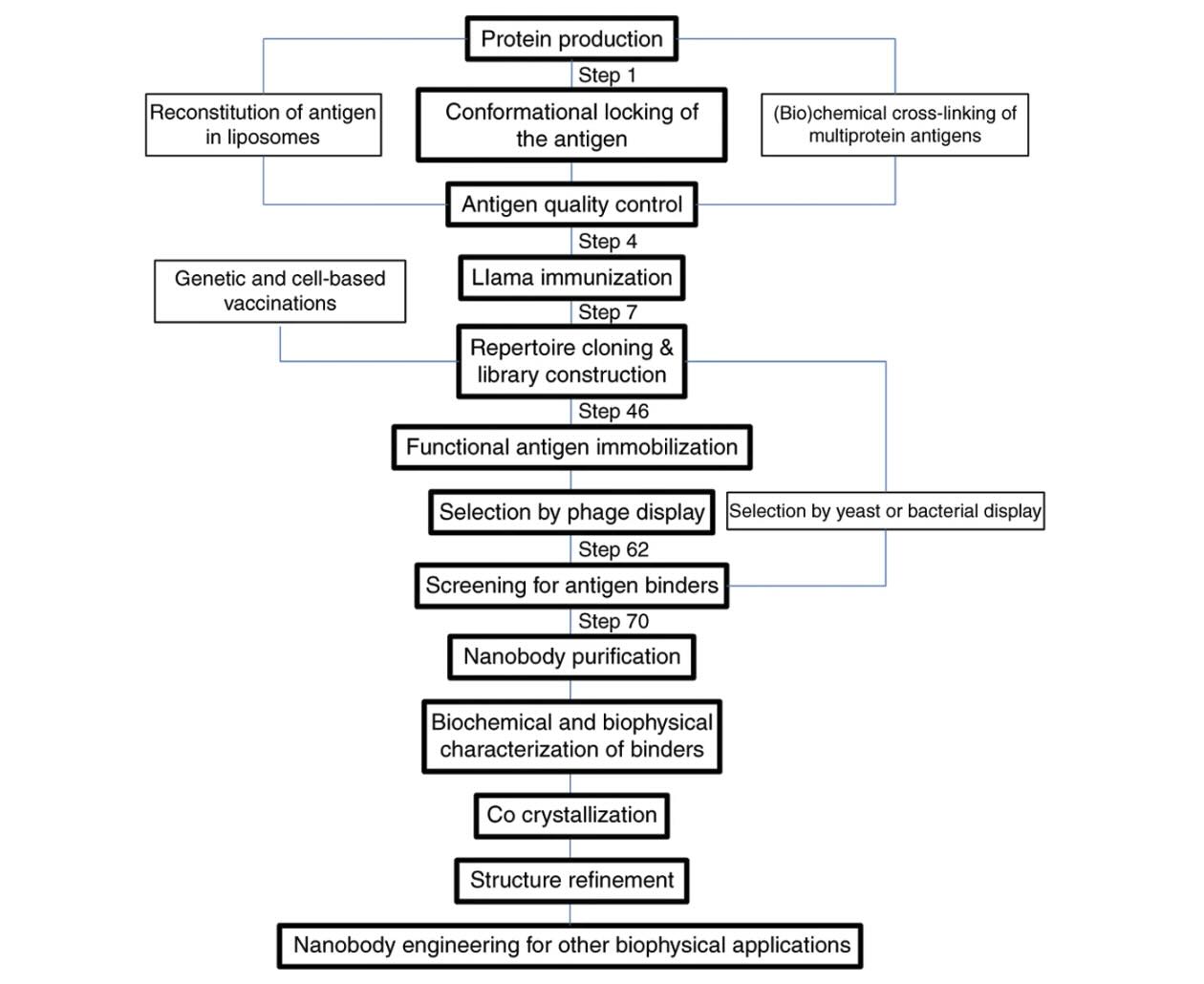
Explore how VHH antibodies stabilize protein conformations for crystallography, ……